Dr. Debasis Maity
Consultant Uro-Surgeon
Medical Discussion
Renal trauma
Remember
- The kidneys = most common genitourinary organs injured from external trauma
- Motor vehicle accidents, falls from heights, and assaults contribute to the majority of blunt renal trauma.
- Direct transmission of kinetic energy and rapid deceleration forces places the kidneys at risk.
- Penetrating renal injuries most often comes from gunshot and stab wounds.
- Bullet size and velocity has the greatest effect on soft tissue damage as predicted by the following equation:
- Kinetic Energy = ½·mass·velocity2
-
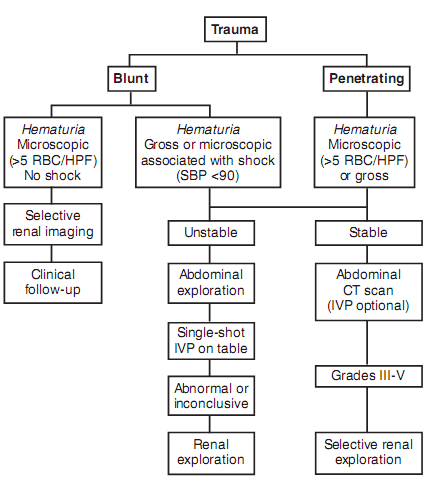
The best indicators of significant urinary system injury =
haematuria- Microscopic: > 5 RBCs/HPF or positive dipstick finding
- Gross hematuria and hypotension: SP < 90 mm Hg
The degree of hematuria and severity of renal injury do not consistently correlate
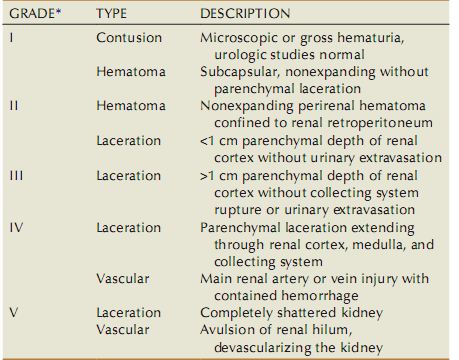
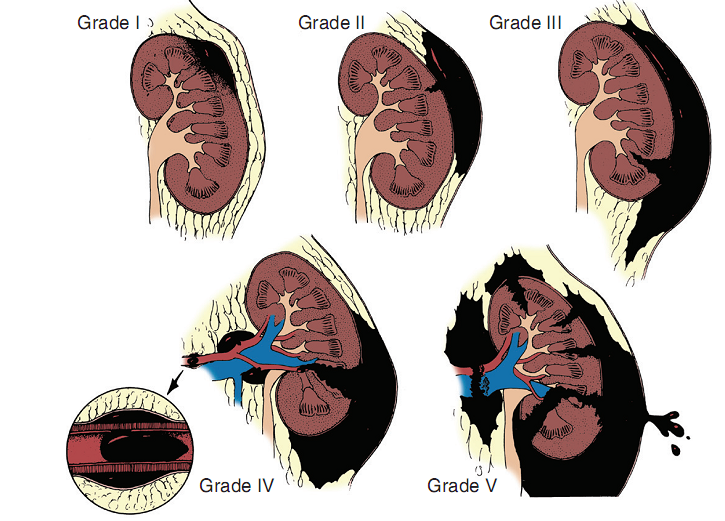
Grade
Indication of renal imaging:
- All penetrating trauma patients with a likelihood of renal injury (abdomen, flank, or low chest) who are hemodynamically stable.
- All blunt trauma with significant mechanism of injury, specifically rapid deceleration.
- All blunt trauma with gross hematuria.
- All blunt trauma with hypotension ( SP < 90 mm Hg) at any time during evaluation and resuscitation.
- All pediatric patients with > 5 RBCs/HPF.
- Patients with microscopic hematuria without shock can be observed clinically without imaging studies.
- Penetrating injuries with any degree of hematuria should be imaged.
Imaging:
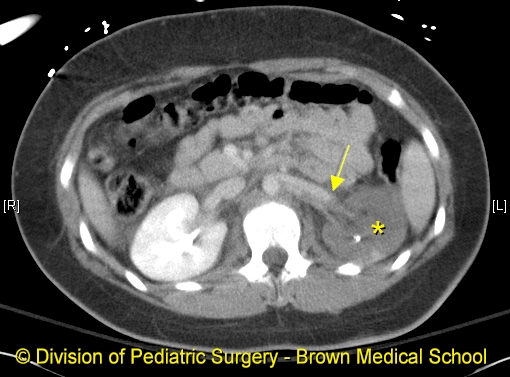
CECT
goldstandard- Highly sensitive and specific
-
Provides most definitive staging information:
- Parenchymal lacerations clearly defined.
- Extravasation of Contrast enhanced urine easily be detected.
- Associated injuries to the bowel, pancreas, liver, spleen, and other organs identified.
- Degree of retroperitoneal bleeding assessed.
- Lack of uptake of contrast material in the parenchyma suggests arterial injury.

- Findings on CT that raise suspicion for major injury:
- Medial hematoma, suggesting vascular injury.
- Medial urinary extravasation, suggesting renal pelvis or ureteropelvic junction avulsion injury.
- Lack of contrast enhancement of the parenchyma, suggesting arterial injury.
IVP:
-
When the surgeon encounters an unexpected retroperitoneal hematoma surrounding a kidney during abdominal exploration.

Management:
Operative management:
- Absolute indications
- Hemodynamic instability with shock
- Expanding/pulsatile renal hematoma
- Suspected renal pedicle avulsion (grade 5)
- Ureteropelvic junction disruption
- Relative indications (rare)
- Urinary extravasation together with nonviable tissue
- Renal injury together with colon/pancreatic injury
- A delayed diagnosis of arterial injury (which most likely will need delayed nephrectomy)
- The management of the intraoperative nonexpanding retroperitoneal hematoma is controversial → Nonoperative therapy is recommended, regardless of mechanism
- Urinary extravasation from grade IV parenchymal laceration or forniceal rupture can be managed nonoperatively - spontaneous resolution > 90%
- Nonviable tissue > 25% with parenchymal laceration or urinary extravasation or both = operative management is recommended
- Segmental renal artery injury with renal laceration results in nonviable tissue (> 20%) → Currently, nonoperative management is favored in hemodynamically stable patientss, although concerns include delayed bleeding and urinoma formation
Renal exploration:
- Surgical exploration of the acutely injured kidney is best done by a transabdominal approach, which allows complete inspection of intra abdominal organs and bowel.
Technique:
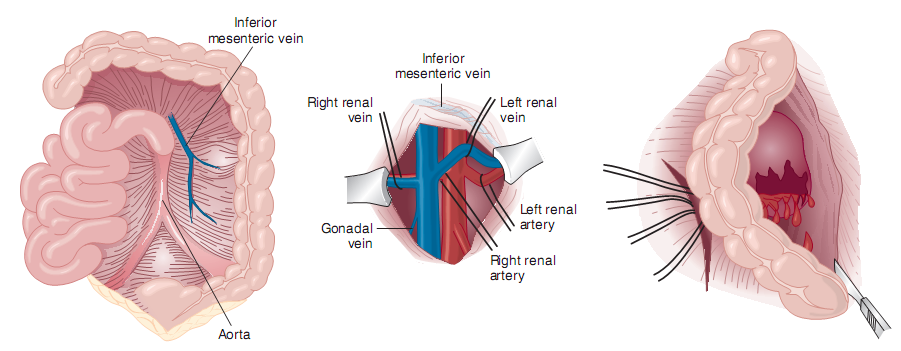
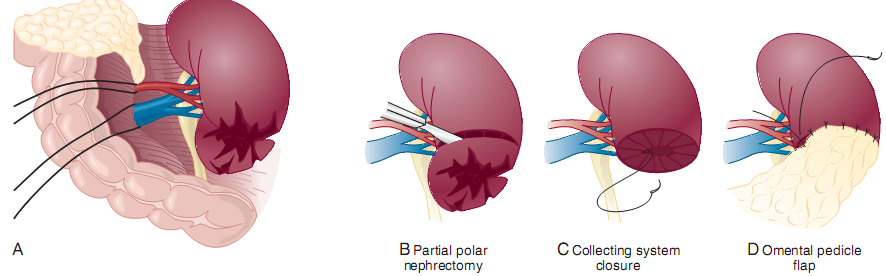
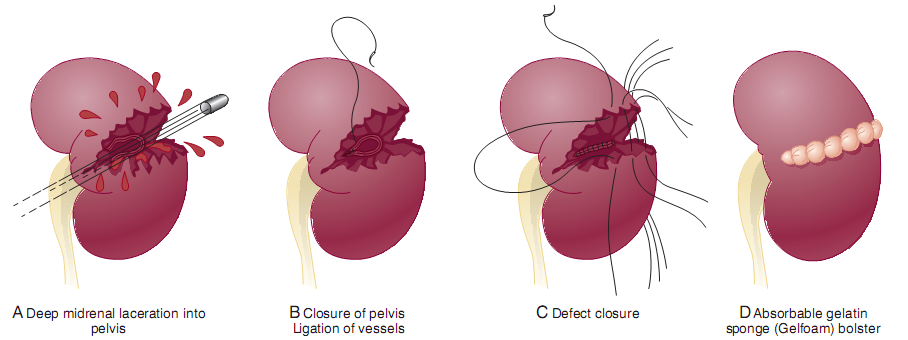
Renal reconstruction:
- The principles of renal reconstruction:
- Complete renal exposure, measures for temporary vascular control, debridement of nonviable tissue
- Hemostasis by individual suture ligation of bleeding vessels
- Watertight closure of the collecting system if possible
- Coverage or reapproximation of the parenchymal defect
- Judicious use of drains
Technique of renorrhapy:
Technique of partial nephrectomy: